Mindfulness Myths in Clinic Life: What’s True, What’s Not, and What to Do Instead
If you’ve ever thought mindfulness means “switching your brain off,” you’re in good company. A lot of smart, capable practitioners carry quiet doubts about it, even if they recommend it to clients.
This post clears up the most common mindfulness myths that get in the way, especially in busy, hands-on clinics. You’ll see what mindfulness is (and isn’t), why some people find it hard to make a start, and how to make it feel practical instead of awkward. Most importantly, you’ll come away with simple ways to talk about mindfulness that keep it grounded, ethical, and easy to try.
Why these myths matter when you’re the practitioner
Misconceptions about mindfulness don’t just confuse clients, they block action. If someone believes mindfulness requires a blank mind, perfect posture, and 20 minutes of silence, they’ll decide they’ve “failed” before they’ve even started.
That matters in clinic because we often offer mindfulness as a small self-care skill. If it feels unrealistic or “not for people like me,” it won’t get used. On the other hand, when you explain it clearly, it becomes easier for clients to try it without pressure.
Myths also affect your working day. When you’re moving from treatment to charting to the next person (with a kettle boil or two in between), you need options that fit real life. You don’t need a whole new routine, you need something that can sit inside the one you already have.
A few practical wins when you clear up the myths:

Myth 1: “Mindfulness means emptying your mind”
A common picture people have is “mindfulness equals a blank brain.” No thoughts, no noise, no mental to-do list popping up at the worst moment.
Here’s the problem: a mind that thinks isn’t broken. It’s doing its job. If your brain produces thoughts during mindfulness, that’s not failure, that’s being human.
Mindfulness is noticing, not deleting. The practice is simply seeing what’s happening in your attention, then choosing what you want to do next. Thoughts can still be there. The difference is that you catch them earlier, with less drama attached.
A clinic-friendly example is charting. You might be writing notes and suddenly notice you’re rushing, or your shoulders are up around your ears, or your inner voice is reminding you of the next client. That moment of noticing counts. You don’t need to stop charting and float off to a mountaintop. You just noticed what was happening.
From there, a useful question is: “Is this helping me right now?” If the answer is no, you can soften your grip, slow your breath, and carry on. You still have thoughts, but they don’t have to drive the bus.
The aim isn’t fewer thoughts. The aim is spotting them sooner, then deciding whether they’re useful.
Myth 2: “Mindfulness is just relaxation”
It would be lovely if mindfulness worked like a spa treatment. Do the exercise, feel calm, drift away from the day. Sometimes mindfulness does feel soothing, but that’s not the main point.
Mindfulness is closer to turning the lights on. You see what’s already there. That includes tension, irritation, worry, and the little flurries of “I should be doing more” that show up when you finally pause.
This is exactly why some people quit. They try mindfulness because they want calm, then they become more aware of what they feel, and they decide it’s made things worse. What actually happened is that their awareness improved before their ability to respond did.
A practical way to describe this to clients is: mindfulness helps you notice what’s happening, so you can make a choice. Calm can come later, but first you need to know where your attention has landed.
If you want to make it feel doable (and less like a “perform calmness” exercise), keep it simple:
- Notice what’s here (thoughts, tension, breath, sensation).
- Name it plainly (“tight chest,” “racing thoughts,” “jaw clenching”).
- Choose a small response (one slower exhale, soften shoulders, feel feet on floor).
That’s it. No forced serenity. No pretending you’re relaxed when you’re not.
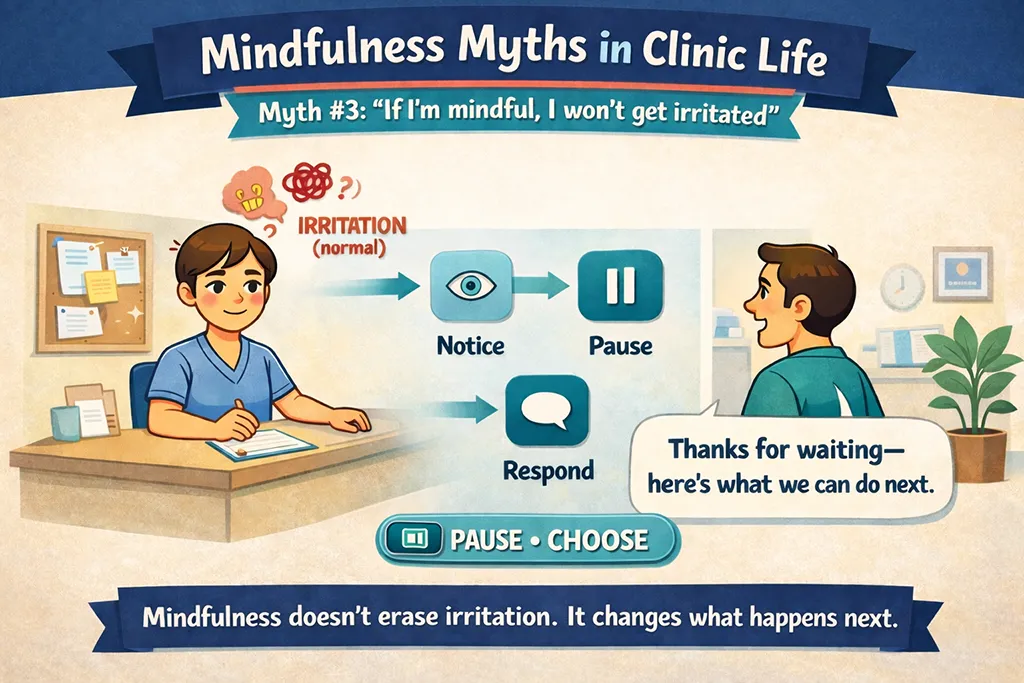
Myth 3: “If I’m mindful, I won’t get irritated”
Many people secretly hope mindfulness will make them permanently nice. No snappy moments, no frustration, no urge to roll their eyes at the person speaking.
Mindfulness doesn’t remove irritation. It can, however, change what happens next.
A helpful way to think about it is “shortening the fuse to action time.” You still feel the irritation, but you notice it sooner. That gives you a gap, just a beat, where you can decide how to respond rather than reacting on autopilot.
That gap matters in clinic life because irritation often leads to habits that don’t support you:
Mindfulness helps you catch the moment before you slide into those patterns. You may still feel the heat of the emotion, but you’re more likely to choose the behaviour you actually want.
In practice, this can be as small as noticing your tone before you speak, or feeling your hand on the door handle before you walk into the next room. The change is often tiny, but it’s real.
Myth 4: “Mindfulness takes 20 minutes a day”
This myth stops people before they start. When someone believes they need 20 uninterrupted minutes daily, mindfulness becomes another task they “should” do, and therefore another thing to fail at.
You can start much smaller.
In a clinic, micro-practices are often the best entry point because they fit between clients. They also feel less emotionally loaded. You’re not sitting down to “fix your mind,” you’re just giving your attention something simple to do for a few seconds.
A few options that work well in real clinic flow:
Those moments might sound too small to matter. Still, they add up. Five minutes scattered through a day can be more realistic than one long session, and consistency tends to beat intensity.
If you want to encourage clients to use mindfulness between sessions, these short practices are also easier to remember. They attach to things people already do, so the habit has somewhere to live.

Myth 5: “Mindfulness means sitting still with perfect posture”
The “perfect posture” myth puts off fidgety people immediately. It also puts off people in pain, because they know they can’t sit still comfortably for long.
Luckily, mindfulness works in motion. The key isn’t the posture, it’s where the attention is.
That means you can build mindfulness into ordinary actions, including ones you’re already doing every day. Walking, stretching, making tea, even cleaning the treatment room can all become mindfulness practice if you bring your attention to the experience itself.
A few simple examples:
For hands-on practitioners, there’s also mindful touch. If you work with your hands, you already have a built-in attention anchor. Feeling the contact, noticing pressure, and staying present with what you’re doing can be an easy way in, both for you and for clients (without adding anything extra to the appointment).
Myth 6: “Mindfulness is spiritual, ‘woo,’ or not evidence-based”
Some clients hear the word “mindfulness” and brace themselves. They expect chanting, incense, or a sales pitch for something that doesn’t fit their world view.
You can avoid that reaction by using plain language and keeping it practical.
Mindfulness, at its core, is about attention training and practising a kinder, less judgmental response to yourself. It doesn’t need any spiritual packaging, and it doesn’t need big promises attached.
If a client is wary, it can help to change the label:
When you keep the language straightforward, it becomes easier for clients to try without feeling like they’re signing up for a whole new identity.
If someone does want to read more about the research side, point them to reputable overviews rather than social media summaries. Two good starting places are the American Psychological Association’s pages on mindfulness and stress, and the UK NHS guidance on mindfulness.
The goal in clinic is simple: help clients understand what they’re doing and why, in words that feel safe and familiar.
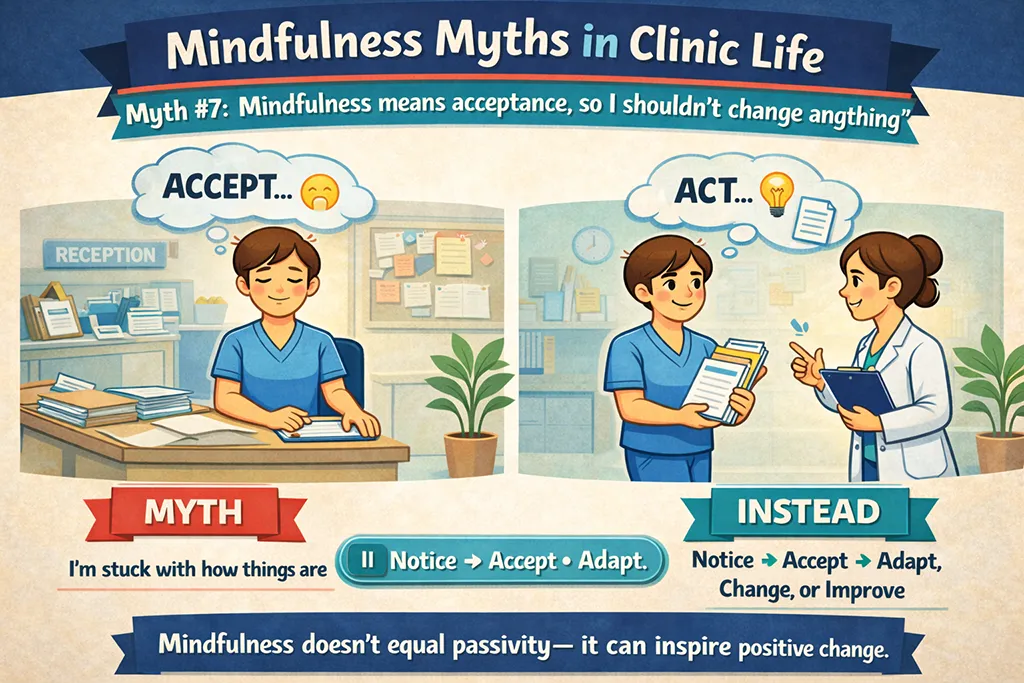
Myth 7: “Mindfulness means acceptance, so I shouldn’t change anything”
This one causes real confusion. People hear “acceptance” and think it means approving of everything, or letting habits run wild because “I’m being mindful.”
That’s not the point.
Mindfulness involves noticing what’s happening, then redirecting attention when needed. Acceptance means you stop attacking yourself for having a mind that wanders. It doesn’t mean you stop making changes.
A simple way to explain it is: your mind wanders, you notice, you bring it back. No scolding required.
This is the difference many clients miss:
|
What mindfulness acceptance looks like |
What it’s not |
|---|---|
|
“My mind wandered, that’s normal. I’ll bring it back.” |
“My mind wandered, I’m doing it wrong.” |
|
“I feel tense. I can choose what to do next.” |
“I feel tense, so nothing can change.” |
|
“I notice the habit, then I decide how to respond.” |
“I notice the habit, so I must keep it.” |
The aim is to name what’s happening without adding a second layer of judgment. You’re not approving or disapproving, you’re simply seeing clearly enough to choose your next step.
Myth 8: “Mindfulness is only for calm people”
Some people assume mindfulness is for the naturally serene. If their brain feels busy, they decide they’re not the right type of person for it.
Busy minds aren’t a barrier. They’re the training ground.
A useful analogy is the gym. You don’t start fit. You go to the gym to get fitter. In the same way, you don’t begin mindfulness with perfect focus. You practise because attention wanders.
The practice is returning, again and again, to something simple: the breath, the feeling of your feet, the sounds in the room. Each return is the skill. If your mind wanders 20 times, you get 20 chances to practise.
For practitioners, this is also a reassuring message to share with clients who say they “can’t meditate.” You can agree with them (because sitting silently can be hard), and still offer a version of mindfulness that fits their life.
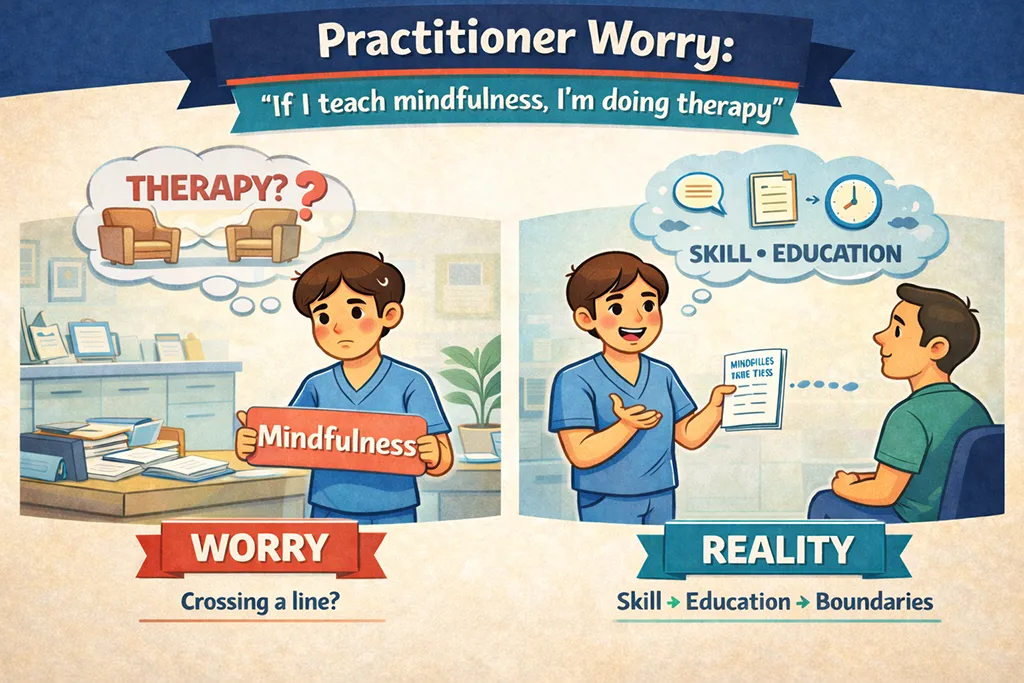
Practitioner worry: “If I teach mindfulness, I’m doing therapy”
This concern can come up in holistic clinics, especially when you care about scope of practice and you want to stay on firm ground.
Offering mindfulness does not have to mean providing therapy. You can share simple self-care practices and in-session exercises that support a client’s ability to settle, focus, and take part in their care.
For example, you might guide a brief grounding exercise before treatment, or suggest a slow exhale while they notice the support of the table. That’s very different from treating mental health conditions, processing past events, or positioning mindfulness as a replacement for appropriate care.
It helps to keep a few boundaries clear:
A grounded way to explain the “why” is this: mindfulness can help the brain and nervous system recover from stress more efficiently, so thoughts, emotions, and symptoms don’t take over as quickly. It’s support, not a full treatment plan.
The ethical sweet spot is mindfulness as a practical skill that supports coping and behaviour change, alongside good clinical care.
Next steps: pick one myth to challenge this week
You don’t need to tackle all of these mindfulness myths at once. Pick the one that has been most sticky for you, or the one you hear most often from clients, and try a small experiment.
If you’ve avoided mindfulness because you thought you had to “do it properly,” try one micro-practice between clients. If you’ve taught it as relaxation, try reframing it as “turning the lights on,” so clients don’t quit the first time they notice tension.
Then, jot down a simple response you can use in clinic when the myth appears. A short line, in plain language, beats a long explanation.
What’s the most common myth you hear, the blank mind idea, the “no time” objection, or the worry that it’s a bit woo? If you can name it, you can answer it, and that’s where mindfulness starts to become useful in real clinic life.
Please Share
Have you got a question that I haven’t answered here? Drop it in the comments. This space is for sharing, not just reading. Sometimes the best advice comes from those who’ve been in the same shoes.
Let’s build a supportive community where no one has to figure it all out alone. And if this helped you today, consider passing it on to a colleague who might need it – a little support goes a long way.
Please pin one of these images to your main business tips board