Imposter Syndrome in Your Solo Clinic: When to Ignore It (and When to Listen)
Imposter syndrome in your solo clinic brings that little voice saying, “Who am I to be doing this?” and it can turn up at the worst times. If you’re a self-employed acupuncturist, massage therapist, physio, chiro, or any other solo health practitioner, you’ve probably met it already. Clinician imposter syndrome is common in solo practice, and it doesn’t always mean anything is wrong.
The trick is learning to tell the difference between fake fear (noise) and a real gap (signal). Once you can sort those two, you stop treating every wobble like an emergency, and you start using the useful bits as a simple map for your own personal and business development.
What imposter syndrome looks like in a solo health practice
Imposter syndrome is that feeling that you’re not good enough, even when your work is good. It’s the mismatch between reality (you’re competent, trained, and trying your best) and the story your brain tells you (that feeling like a fraud, you’re about to be found out, any minute now).
It’s also important to say what it isn’t. Imposter syndrome is not the same thing as being untrained, unsafe, lacking clinical competence, or working outside your therapist role. Those are real practice issues, and they need real action. Imposter syndrome is more slippery, it often shows up when you’re actually doing fine.
In a clinic, it can look surprisingly ordinary. You might notice it when you:
And yes, persistent self-doubt often clusters around the practical stuff: pricing, marketing, boundaries, and all the business basics that may not have been taught to you in clinical training.
I had my fair share of imposter syndrome. It was loudest in the first six months of practice but it would come back to nag at me from time to time well beyond that. My imposter syndrome took the form of each of those clinic views above; overpreparation, fear of being found out, all of them.
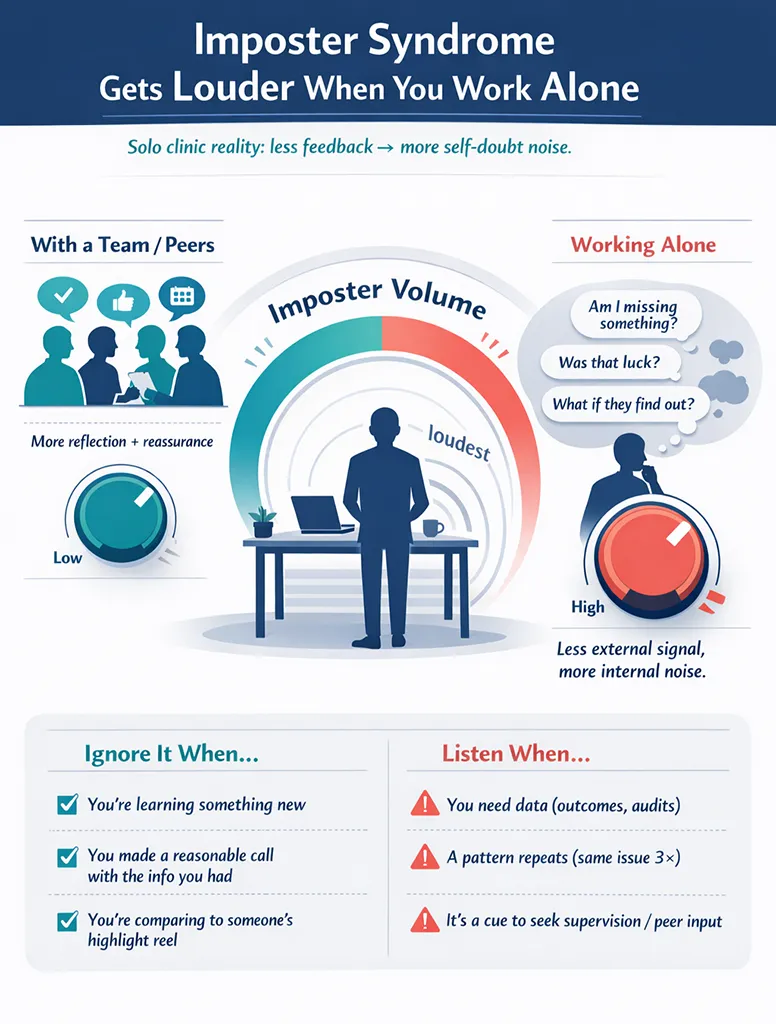
Why imposter syndrome gets louder when you work alone
Working alone in private practice can turn imposter syndrome up to maximum volume, even if your clinical work is solid.
For one thing, there’s no team around you to reality-check your thinking. In training, you had feedback loops built in. In employed roles, you had peer support from colleagues, supervisors, and casual “How would you handle this?” chats. As a soloist, you’re the clinician, receptionist, bookkeeper, marketer, and the complaints department (even when nobody is complaining, your brain still likes to prepare a speech).
Comparison doesn’t help either. You see your own messy behind-the-scenes. You see other clinics’ highlights. Their tidy Instagram grid does not show the late rent payment, the awkward client conversation, or the fact they also rewrote an email five times. This contrast amps up internalized pressure.
Be very careful of that. Comparison is a fast way to talk yourself out of perfectly good decisions.
And one more factor that matters: when you’re tired, your brain tells dramatic stories. A normal cancellation becomes “Everyone hates me.” A slow week becomes “I’m a fraud.” It’s not a character flaw, it’s just a human nervous system trying to keep you safe by scanning for danger.
The two types of imposter feelings: noise vs signal
Not all imposter thoughts deserve the same response. Some should be ignored. Some should be used.
A simple way to sort it is to think of two types of data: noise and signal.
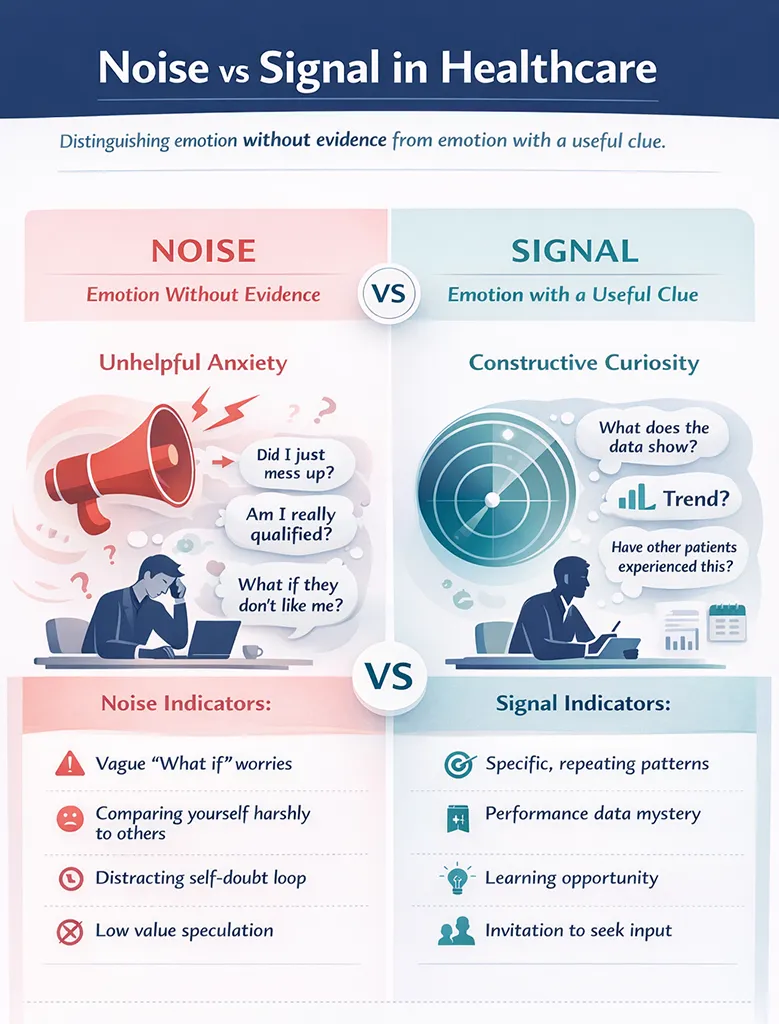
Type 1: The noise (emotion without evidence)
Noise is that shaky feeling that you’re behind, but you can’t actually name what you’re lacking.
It often pops up right after something uncomfortable happens, like:
Noise loves vague panic. It pushes you toward spirals like, “I’m not good enough,” without offering a single practical next step.
That’s the giveaway. Noise is loud, but it’s not helpful.
Type 2: The signal (emotion with a useful clue)
Signal feels uncomfortable too, but it comes with something solid you can point to.
It sounds more like:
Signal is still a bit annoying (fine), but it’s useful. It tells you exactly what your next support step should be, whether that’s training, supervision, a script, a template, or a clearer referral plan.
How to check which one you’re dealing with
When that “imposter” feeling shows up, pause and run a quick internal check:
If it’s vague panic, treat it as noise. If it’s a clear, nameable gap, treat it as signal.
One of the things that helped me to sort the noise from the signal was investing in supervision (more of a mentoring and coaching service). I joined a supervision group and that’s where I found reassurance that I wasn’t alone in the feelings of “who am I to do this”.
When you should ignore imposter syndrome completely
Some imposter thoughts aren’t messages. They’re just nerves in a trench coat.
Here are the situations where it’s usually best to ignore imposter syndrome (and carry on anyway).
Right after you’ve done something brave
If you’ve just raised your fees, posted on social media, improved your Google presence, launched a program, or started asking for reviews, you may feel nervous about reactions. That’s normal.
Doing something new often triggers a “Who do you think you are?” response in your body. That doesn’t mean the decision was wrong. It often means it mattered.
When it’s based on comparison
Maybe another clinic looks fancier than yours. Maybe other practitioners post confident videos and you’re still trying to work out what to say, and how to say it without sounding like a robot. Comparison often stirs up fear of failure.
Confidence is not proof of competence. It’s often just proof of practice.
When your outcomes and feedback are genuinely good
This one’s important. If clients are rebooking, referring friends, and telling you they feel better, pay attention to that positive feedback.
Your brain may still try to argue, but client outcomes and trust count for a lot.
When it’s really fear of visibility
Visibility nerves can look like imposter syndrome: fear of being seen online, being listed publicly, or asking for reviews.
If you notice that your worry spikes around how you’re being perceived (rather than around a clinical skill), treat it as a normal fear response, not as a verdict on your ability. Visibility is not dependent on external validation.
What to do instead of spiraling
You don’t need a giant self-improvement project. Try a few small anchors:
Keep a success file where you can find it quickly. Save kind messages, feedback, wins, and results. On wobbly days, you need receipts.
Make one decision per day without running it past six people. Build your own trust muscle.
Follow your scope, your notes, and your consent process, then stop replaying the session. Running it over and over feels like “being responsible,” but it rarely makes you better.
If you want a simple way to steady the business side (so fewer things feel like a personal failing), a simple business plan for solo health practices can help you separate “my clinic systems need work” from “I’m not cut out for this.”

When you should listen: real gaps, boundaries, and patterns
Sometimes that niggly voice is pointing to something real. Not a moral failing, just a gap you can close.
Listen more closely when the feeling points to a specific skill, scenario, or boundary issue, such as:
You avoid certain cases because you don’t feel grounded in the basics. You might find yourself hoping they don’t book, or feeling a sinking feeling when they do.
You freeze when a client asks about progress, timelines, or next steps, the classic expert trap. You go vague in your explanation because you’re not sure what to say.
You catch yourself thinking, “I hope nobody asks me about that.” (That sentence is often a clue, even when you try to laugh it off.)
You feel stretched past the end of your scope. That’s not imposter syndrome, that’s a boundary moment. In that situation, the best move might be to refer out, co-treat, or get clinical supervision.
You notice a pattern: the same client type, the same trigger, the same moment in the session where you feel wobbly. Examples might include chronic pain clients with lots of questions, athletes who want firm timelines, or clients with trauma history that need careful handling.
And if you’re running on very low energy, be cautious with your self-assessment. A tired practitioner feels vulnerable and doubts everything, even the basics. Before you decide you’re “bad at this,” consider whether you simply need rest, fewer decisions, and more support around your workload.
How to use imposter syndrome as a practical map (without buying random courses)
When imposter syndrome is a signal, the goal isn’t to silence it with reassurance. The goal is to turn it into one clear action.
Step 1: Turn the anxiety into one clear sentence
This matters more than it sounds. Vague fear stays stuck. A clear sentence can be solved.
Try:
Short, plain, and specific.
Step 2: Sort it into a useful bucket
This is how you avoid late-night panic decisions and training that doesn’t match the problem.
Here are four buckets that cover most solo clinic wobbles:
|
Bucket |
What it often includes |
What “support” might look like |
|---|---|---|
|
Clinical skills |
assessment, technique choice, red flags |
training, supervision, case consultation, case discussion |
|
Communication skills |
explaining plans, setting expectations, boundary talks, professional identity |
scripts, role-play, supervision, practice |
|
System skills |
intake process, note-writing, policies |
templates, checklists, updated forms |
|
Business skills |
pricing, packages, scheduling, marketing basics |
simple plan, small experiments, tracking |
Once you’ve named the bucket, you can look for the smallest thing that will actually fix it.
Step 3: Find the smallest support that solves the problem
Small does not mean trivial. Small means targeted.
That might be:
A supervision session focused on one tricky case type.
A short course that teaches one clear skill.
A template for your notes, intake, or policies.
A colleague swap where you review each other’s policies, scripts, or websites (two smart clinicians, one cup of tea, 30 minutes, done).
Step 4: Make a tiny practice plan and add one guardrail
Now, with a growth mindset, test the new skill in a controlled way.
Use it with your next three suitable clients. Keep notes on what worked. Save your script so you don’t reinvent it each time.
Then add one guardrail, something like: “If this case is outside my comfort zone, I’ll refer it or co-manage.”
Guardrails reduce stress fast, and they keep care safe.
Real clinic scenarios: should you ignore it or use it?
It helps to see what this looks like in real life, not just in theory.
Scenario 1: You raised your fees and feel slightly nauseous
Ignore it.
Hold your prices for 60 days. Track bookings and re-bookings during that time. You’re looking for evidence, not a mood. After 60 days, review and adjust if needed, but don’t change prices every time your nerves speak up.
Scenario 2: A client asked a question and you stumbled
Use it.
That stumble might stir up fear of failure. Write a short script for that exact question, then practise it out loud twice. Often you only stumble because it’s the first time you’ve had to explain it in a while.
Also decide: do you want to treat this type of case? If not, refer them to someone better suited. That’s good practice, not failure.
Scenario 3: You dread a certain type of case
Use it.
Decide whether you want this case type on your service list.
If yes, get supervision or extra training, and build confidence through repetition.
If no, tighten your intake screening so fewer of these cases book in the first place, and set up a clear referral path.
Scenario 4: Your week is slow and you think, “I’m a fraud”
Ignore it.
A slow week happens in healthcare, and it can amplify that feeling like a fraud. Holidays, weather, school runs, money cycles, and random life events can all affect bookings.
Do a quick systems check instead: your Google profile basics, your review process, and your rebooking habits. Then move on with your day.
Scenario 5: You keep giving away extra time
Use it.
That’s often a sign you need a boundary script and a clear policy (for follow-ups, texting, or over-running sessions). Set the rule when you’re calm, not mid-session when you feel cornered.

What not to do when imposter syndrome shows up
A few common reactions make imposter syndrome worse, even though they feel productive in the moment.
Don’t treat imposter syndrome by collecting endless certificates, a common pitfall for high achievers. More training can be great, but only if it matches a real, nameable gap and is also a service you want to provide.
Don’t use “I’m not ready” as a permanent parking spot. Let it be a moment, not a home address.
Don’t ask ten people for reassurance. You’ll get ten different opinions, then feel worse. Practice self-compassion as an internal anchor instead.
Don’t confuse “I’m nervous” with “I’m not allowed to do this.” Nervous is a feeling. Scope is a fact.
Support can help, of course. Clinical supervision, peer groups, and coaching all have their place. Just keep the support targeted to the signal, not the noise.
A calmer next step you can take this week
Overcoming imposter syndrome in your solo clinic doesn’t go away because you shame it into silence. It eases when you treat it like data, sort the noise from the signal, and take one small action.
Pick one area that triggers that “not good enough” feeling. Write it as a single sentence. Choose one small support step to match it, such as positive feedback, one script, one template, one supervision chat, or one guardrail.
Then let that be enough for now. You don’t need to fix everything at once, you just need to keep moving in the right direction.
Please Share
Have you got a question that I haven’t answered here? Drop it in the comments. This space is for sharing, not just reading. Sometimes the best advice comes from those who’ve been in the same shoes.
Let’s build a supportive community where no one has to figure it all out alone. And if this helped you today, consider passing it on to a colleague who might need it – a little support goes a long way.
Please pin one of these images to your main business tips board