Clinical Decision Confidence: How to Make Clear Decisions Without Second-Guessing Yourself
As a solo healthcare professional, making decisions in clinic can feel harder once you’re on your own. Not because your training vanished overnight, but because you’ve lost the sounding board that used to come with it, which can erode your clinical decision-making confidence.
This post is about building clinical decision confidence without spiralling into “Was that the right call?” after every session. You’ll learn why solo work makes second-guessing more common, what usually triggers it, and a simple five-step process (CLEAR) you can use today to choose a plan, act on it, and review it properly.
Why solo health providers get stuck in decision loops
Solo practice asks you to make a lot of decisions, back-to-back, with no pause and no colleague at the next desk. In training, you probably had case chats built into your day. You could test your thinking out loud, hear another approach, and leave feeling more grounded.
Then you open your own clinic after having had supervised work experience and it’s just you, the client, and that quiet little voice that says, “Hmm… should I have done something else?”
It’s also not just clinical decisions anymore. You’re also deciding:
That mix creates decision fatigue, which can make even simple choices feel heavier than they should. The aim is not to become some sort of unshakeable robot. It’s to use a simple process that supports your thinking, so you can make a call, test it, and learn from what happens next.
What you lose when you leave training
The tricky part isn’t that you stop knowing things. It’s that you stop getting that steady drip-feed of feedback from your peers.
While working through your education, discussing cases helps you build pattern recognition. You also learn what “normal uncertainty” feels like. In solo work, uncertainty can feel like a warning sign, even when it’s just part of practice, and development shifts to self-directed learning.
If you want to replace that support, formal clinical supervision can help (more on that later). If that’s not possible right now, you can still build structure into how you decide, which makes the day-to-day feel steadier.
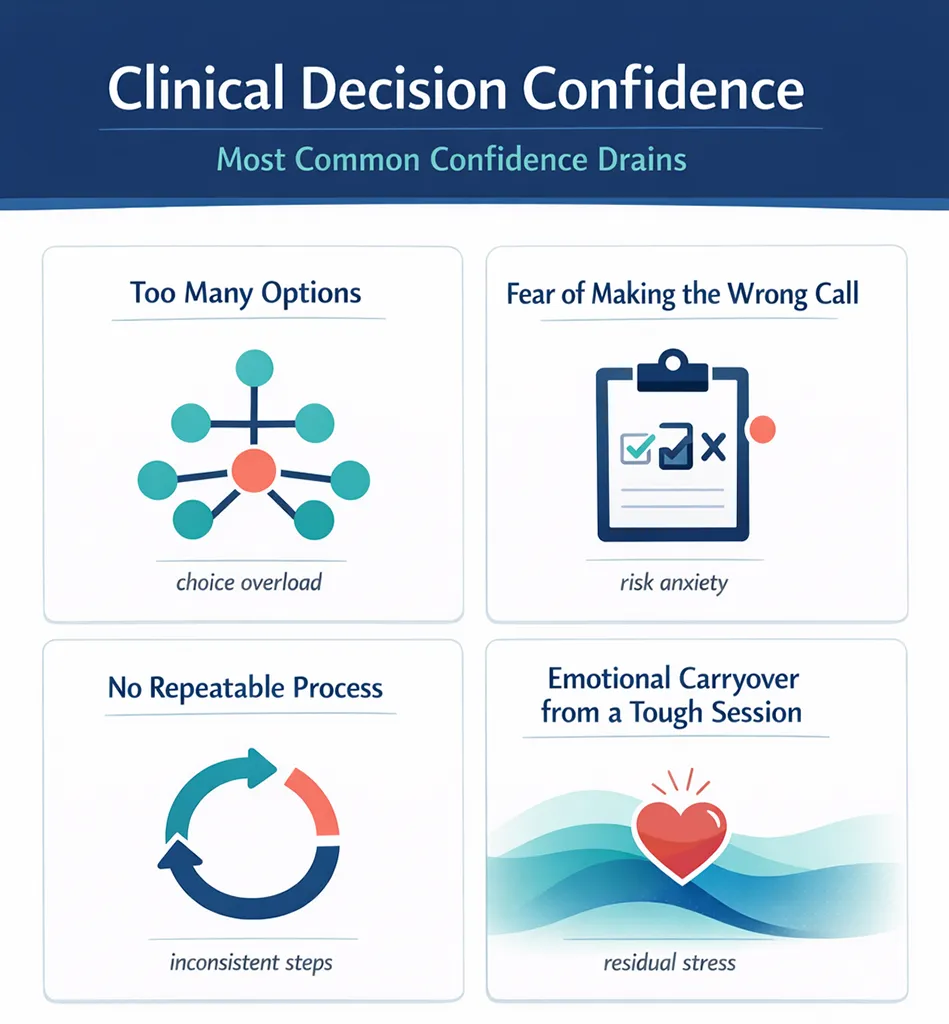
The most common confidence drains (and why they bite)
Second-guessing usually doesn’t come from one dramatic moment. More often, it comes from repeatable situations that nudge you off balance. Here are four that show up a lot in solo practice, draining your clinical decision-making confidence.
- Too many options
- Fear of making the wrong call
- No repeatable process
- Emotional carryover from a tough session
Each one has a simple fix, but first you need to spot which one you’re dealing with.
Too many options makes decisions harder, not easier
Having lots of tools is great, right? Until you have to pick one, in real time, with a client watching your face for clues.
More options can lead to more second-guessing, because every choice also means rejecting ten other choices. It’s the same reason clients can freeze when you offer a menu of six appointment types. It sounds helpful, but it can make decisions feel risky.
In clinical work, “too many options” might look like:
None of those are bad. The problem is trying to keep them all equally available at all times. You don’t need fewer skills. You need fewer active choices in the moment.
Fear of the wrong call keeps you stuck
The fear is usually not “I might make a small mistake.” It’s bigger than that. It’s “What if this makes them worse?” or “What if they don’t come back?”
Here’s the truth that’s both annoying and freeing: the “wrong” call for one client is not the wrong call for another. You’re not choosing the perfect plan for all humans. You’re choosing the best next step for this person, today, based on what you see and what they can do.
That said, one fear is worth treating with real respect: missing something serious and compromising diagnostic accuracy or patient safety. Knowing your red flags and your personal “worry spots” helps a lot, because it draws a clear line between:
When you trust your red-flag knowledge, the rest of the decision feels less loaded.
If you see a red flag, the next step is referral, not debate.
No repeatable process means you never collect useful evidence
If you change your approach every session, it becomes almost impossible to trust your own thinking. Not because you’re doing it “wrong”, but because you never give anything long enough to show you whether it works and you fall prey to cognitive bias.
A repeatable process doesn’t mean rigid care. It means you can answer basic questions like:
Without that, every session starts from scratch. You spend more time deciding and less time doing.
Repeatability also makes your notes clearer, your re-assessments sharper, provides clinical decision support for your future decisions, and speeds them up (because you’re building a library of real-life results).
How to stop one tough session from hijacking the rest of your day
One intense appointment can colour everything that comes after it. Maybe a client cried. Maybe they got angry. Maybe they challenged your plan, or reminded you of a past case that didn’t go well.
Those reactions can stick to you like a burr on a wool jumper. You move to the next client, but part of your brain is still replaying the last session.
A simple fix is to build a reset between sessions. Nothing fancy. Just something that tells your body, “That one is done.”
And keep this phrase close by:
Feelings are data, not directions.
In other words, your reaction contains information. It might tell you a boundary got pushed, a topic hit a nerve, or you need to explain your plan more clearly next time. Still, it doesn’t get to steer your whole day.
The CLEAR framework for confident clinical decisions
When you’re working solo, you need a process you can run in your own head, quickly, without turning every case into a philosophy essay.
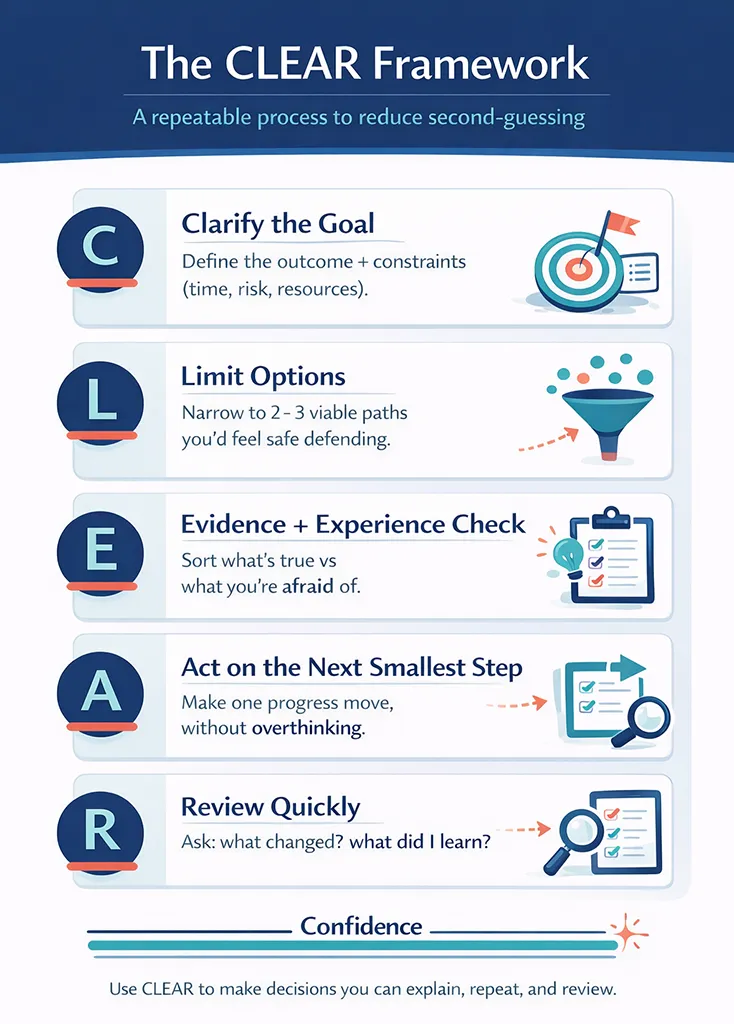
Here’s a five-step framework you can use to build your own clinical decision-making confidence: C-L-E-A-R.
It helps you get clear on the goal, reduce your choices, check the facts, take a small step, and then review what happened. This clinical reasoning builds self-efficacy and confidence.
C: Clarify the goal (and the constraints)
Start by naming what you’re trying to change. Keep it practical and observable. Then name what you need to respect, because constraints are real life, not inconveniences.
Outcome examples:
Constraint examples:
This step stops you chasing ten goals at once. It also stops you planning a gold-standard programme for someone who can realistically only manage the bronze version right now (and that’s fine).
L: Limit options to two or three viable paths
Next, reduce your choices on purpose. Aim for two to three reasonable options, not the full catalogue of everything you can do.
Fewer options makes it easier to compare trade-offs and easier to notice results. It also reduces the urge to keep switching approaches too soon.
Here’s what that can look like:
|
Viable path |
What it focuses on first |
When it can fit well |
|---|---|---|
|
Path A |
Symptom relief, then rehab |
When pain is high and the client needs early wins |
|
Path B |
Graded exposure now, lighter hands-on |
When the client can tolerate gradual loading and wants an active plan |
The key is that both are sensible. You’re not picking between “good” and “bad”; you’re choosing the best match for personalized therapy to this client’s needs and capacity today.
It also helps to bring the client into it. You can say, “We’ve got a couple of good options, here’s what each looks like.” That keeps the plan clear without dumping every possible technique in their lap.
Client readiness matters here. If someone is in a lot of pain, lifestyle changes might be a future conversation, not today’s homework. You can still mention them, then park them kindly until the client has space to act on them.
E: Evidence and experience check (facts vs fear)
This step separates what you know from what you worry.
Ground your choices in evidence-based medicine by looking at your evidence:
Useful questions include: Have they had this before? What helped? How long did it last? How long until symptoms crept back?
Now compare that to the fear story, which often sounds like:
Fear speaks in absolutes. Evidence usually doesn’t.
Also, keep the boundary clear: if you spot a red flag here, this step ends in referral. No internal arguing required.
A: Act on the next smallest step
Now decide what to do, but keep it small enough for real-time assessment so you can learn from it.
Try one technique, not five. Give one home task, not a complete life overhaul. Book a shorter re-check if you can, so you get feedback while the signal is still clear.
You don’t need the whole plan today. You need the next step, taken on purpose.
R: Review quickly, then decide what’s next
Confidence comes from seeing the link between action and outcome. That only happens when you review while you still remember what you did and why.
Keep the review tight. These three prompts work well:
- What changed since last time?
- What did I learn about the pattern?
- What will I do next because of that?
This is also where focus helps. If you tend to see the same types of clients regularly, patterns show up sooner, and your decisions get easier. You’ll know faster when to stay the course and when to pivot.
On the business side, a simple plan also reduces the number of daily choices you have to make. If you want a practical way to get that clarity, this guide to a simple business plan for health practices fits nicely alongside CLEAR, because it helps you decide what matters, and ignore the rest.
Support structures that make solo decisions easier
CLEAR works even when you’re on your own. Still, it’s worth saying out loud: you don’t have to do everything alone just because you’re self-employed.
One option is clinical supervision. In early practice, group supervision can be especially helpful. You meet with a supervisor (often monthly), bring tricky cases, and talk through both clinical decisions and the practical mechanics of running a clinic. It recreates some of what training gave you, but with real-world cases and real-world business problems.
If supervision isn’t on the cards right now, you can still build support through habits:
None of this is about becoming rigid. It’s about making your decisions easier to trust.
I’ll be honest, I didn’t want to spend the money on supervision when I first finished training and moved into practice. After a couple of months on my own though I started to see the true value. It wasn’t that I couldn’t cope on my own but it did remove a whole bunch of second-guessing. Over time, it also helped me to make the shift from working with peer feedback to customer feedback (the evidence base).
Your next steps (so you can decide, act, and move on)
Second-guessing doesn’t mean you’re bad at what you do. It usually means you’re trying to think clearly without enough structure or feedback.
Pick one case this week and run CLEAR on it, start to finish. Keep the options to two or three, take the next smallest step, then review quickly. After a few rounds, you’ll have something better than reassurance, you’ll have evidence from your own work, strengthening your clinical decision confidence.
Trust your training, trust your ability to adapt, and most of all, trust what you observe in front of you. That’s where good decisions come from, one clear step at a time.
Please Share
Have you got a question that I haven’t answered here? Drop it in the comments. This space is for sharing, not just reading. Sometimes the best advice comes from those who’ve been in the same shoes.
Let’s build a supportive community where no one has to figure it all out alone. And if this helped you today, consider passing it on to a colleague who might need it – a little support goes a long way.
Please pin one of these images to your main business tips board